Mitral valve controls unidirectional flow between the left atrium and the left ventricle. That is is undoubtedly one of the most complex heart structures because its function is a part of the valve itself, dependent on the left ventricle function. The valve closes during the myocardial contraction – systole, that ejects the blood into the aorta. During the myocardial relaxation phase – diastole, the mitral valve widely opens to provide the left ventricle filling.
Rheumatic mitral stenosis was the leading cause of the mitral valve disease. The widespread antibiotic use significantly reduced the incidence of rheumatic fever in developed countries. Therefore, the degenerative valve disuse becomes the primary mitral valve pathology today.
Valve tissue degeneration leads to the chordal elongation and rupture. Mitral leaflets are not closing correctly during the systole; therefore, allowing a portion of blood to regurgitate back into the left atrium. The left ventricle gets volume overloaded, dilates, and eventually fails. The main symptoms of mitral insufficiency are shortness of breath on effort, fatigue, and rhythm disturbances. Rest or supine position dyspnea are signs of advanced disease.
The second most common cause of mitral insufficiency is coronary artery disease due to myocardial infarction.

Mitral valve regurgitation is manly repaired today. Grace, to its anatomy it is possible to reshape the mitral valve tissue, making it functional without prosthesis implantation. Mitral valve reconstruction is the golden standard in degenerative mitral insufficiency. Repaired mitral valve patients do not need lifetime anticoagulation therapy and have less postoperative complications. The experienced surgical team could repair more than 95 to 98 % of degenerative mitral valves. In ischemic mitral valve insufficiency or rheumatic mitral disease, the repair is possible, although it is less feasible and has limited durability.
If impossible to repair, the mitral valve is replaced, of course, either with mechanical or tissue prosthesis. Mechanical valves are durable but require lifetime anticoagulation therapy. Tissue valves are less durable, but patients need no lifetime anticoagulation therapy and, therefore, used in patients over 65 years.
Mitral valve REDO operation
Astic Hasim, 67 years, Sarajevo, Bosnia and Herzegovina.
Mr Asotic sufered from severe mitral regurgitation due to huge dechiscence of previously implanted mechanical mitral valve prosthesis. He vas rejected for surgery from several hospitals due to signifacant operative risk, that was estimated above 30 % according to EUROSCORE 2 scale. Eventually, he was accepted for surgery and operated at Cardiocascular Institute „DEDINJE“ in Belgrade, Serbia by Prof Stojanovic Ivan. His prosthesis was replaced by a new one along with two aortocoronary bypasses. After few weeks of ICU recovery Hasim was dicharged form the hospital with implanted pace maker as well.
After postoperative recovery and COVID-19 pandemic shutdown Hasim returned to his craftsmen shop in famous Sarajevo bazzar of Baščaršija.

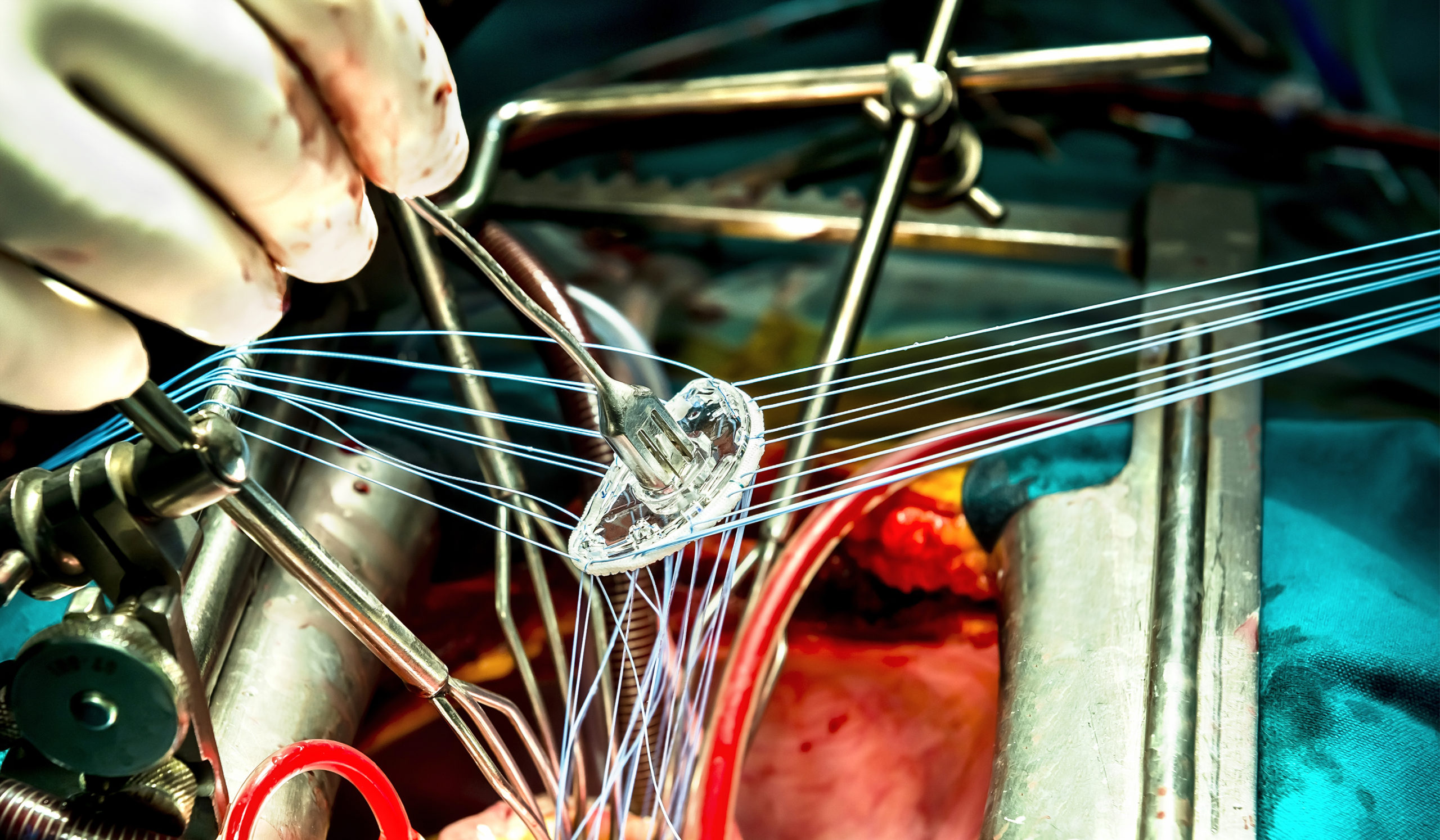
The first mechanical valve prosthesis
The first mechanical valve was implanted on 21st September 1960 by doctor Albert Starr, who designed it all together with engineer Mr. Lowell Edwards. This valve operated like a ball in a cage, similar to kids snorkels. The so-called Starr-Edwards prosthesis has been successfully implanted in more than 300 000 patients and reported to be functional in some patients more than 30 years after implantation. Meanvalve, the valve has been replaced by superior leaflet valves.
MITRAL VALVE REPAIR
Mitral valve repair is a surgical procedure in which we reconstruct the mitral valve to restore its function. We preserve mitral valve leaflet tissue, and the only foreign material implanted is an annuloplasty ring, which is necessary for repair stability and durability. Several different surgical techniques are available nowadays to retail or reshape the mitral valve, making it fully competent.
Degenerative disease is the leading cause of mitral insufficiency today. Loss of collagen and elative fibers are the main features of the disease. Tendinous chordae gets elongated, therefore, and eventually rupture, leading to an incompetent valve that is regurgitating blood back into the left ventricle. That is is what we call the mitral leaflet prolapse. Insufficiency results in heart volume overload, heart chambers get dilated, and the myocardium began to fail over time. The left atrium enlarges as well, and arrhythmias, mainly the atrial fibrillations, appear meanwhile.
Postoje izolovani prolapsi prednjeg ili zadnjeg mitralnog listića kao i udruženi prolapsi oba listića. U osnovi prolapsa leži degenerativna bolest vezivnog tkiva zalistka, odnosno gubitak kolagenih ili elastičnih vlakana.
Pregnancy after mitral valve repair
Marija Mitić, pregnancy after mitral valve repair
Pregnancy is possible but risky though after the valve replacemt with mechanical prosthesis due to teratogenic effects of Coumadine. This is why is important to make any effort to repair in women of childbearimng age. Marija Mitić is one of many weomen who had safe pregnancy and delivery due to mitral valve repair surgery

MITRAL VALVE REPAIR BENEFITS
When compared to the replacement, the mitral valve repair has superior short- and long-term survival. Mitral valvuloplasty is superior to the replacement in terms of postoperative complications as well. Patients experienced less hemorrhagic, thromboembolic, and infective events postoperatively. Since there is a minimal amount of the foreign body implanted, the mitral valve repair patients need no lifetime anticoagulation therapy. Coumadin based drugs, therefore, are taken only during the first three months after the surgery.
Mitral insufficiency is operated in the early stages of the disease if there is a high probability for the repair. An experienced surgical team with a high volume of mitral repairs performed annually is the best choice for the success of the procedure.
Repair durability in degenerative mitral valve prolapse is excellent, though, with 90 – 98 % of repaired valves fully functional twenty years after the surgery. In non-degenerative valve disease, the mitral repair is less durable. For example, around 70 % of rheumatic valves repaired are functional 15 years after the surgery. In ischemic mitral disease, the repair possibility and durability are highly dependent on the left ventricle dysfunction, leading to 30 % of the repair failure within six months after the surgery. The decision of repair or to replace such a valve depends on surgical experience, left ventricle dysfunction, and valve anatomy itself, and should be fully cleared with the patient preoperatively.
MITRAL REPAIR PATIENTS STORY
Alexander Lodjinović, pilot, mitral valvuloplasty
Alexander underwent mitral valve repair due to a severe degenerative mitral valve disease. If replaced, Alexander will lose flying clearance and his job as well. Professor Ivan Stojanovic operated on him at Cardiovascular Institute “DEDINJE” in Belgrade. One year later, he successfully passed a pilot medical exam in the USA, and renew full flying clearance. Today he is still flying for an international airline company.

ENDOSCOPIC MITRAL VALVE REPAIR
“Port – access” surgery is a less invasive cardiac surgery procedure in which we use endoscopic techniques to operate the heart through a small chest wall incision. Although mainly used for the mitral valve repair surgery, but tricuspid valve, some congenital defects, and heart tumors could be removed this way as well.
Port access procedures are performed through a small, up to 5 cm short surgical is made an incision over the fourth left intercostal space below or through the nipple. Another tiny incision is necessary for endoscopic camera placement and up to 3 cm groin incision for cannula placement. Chest wall cuts are in the breast fold anterolaterally and hardly visible after the surgery. By such a minimally invasive approach, we avoid cutting the chest bone, which significantly decreases the trauma. In addition to extraordinary esthetic results, patients who operated that way have less pain, minimal blood loss, and faster recovery after the surgery. For example, patients who are operated through the median sternotomy have to sleep in a supine position during the six weeks after the surgery, while port – access patients are fully mobile after that and regain complete physical and professional activity within 2 – 3 weeks the procedure.



The mitral valve repair is of the highest importance for patient well-being. Therefore, small incisions and less traumatic approaches are justified if there is a high probability of valve reconstruction. It is essential to talk to your surgeon about your mitral valve disease, body anatomy, and clinical status to choose the best option for you.
ANTICOALGULATION
Of course, anticoagulation is mandatory in valve replacement surgery if with the mechanical prosthesis. Otherwise, anticoagulation drugs are necessary three months after the mitral valve repair if no other medical condition exists. During that time, heart tissue will cover the annuloplasty ring. In the case of atrial fibrillation, lifetime anticoagulation is mandatory regardless of successful mitral repair.
Three months after the surgery, an ECG and cardiologist check-up is necessary to stop the anticoagulation drugs. Patients should not stop taking anticoagulation therapy by themselves. Otherwise, they risk catastrophic complications.
This site is for education purposes only. The author of the site disclaims no responsibility in case of inappropriate treatment. Therefore, patients have to consult their physicians for further therapy.
FIRST ENDOSCOPIC HEART SURGERY IN SERBIA
The first endoscopic heart surgery in Serbia was performed by Prof Ivan Stojanoivć and his team on 21st December 2011. That was the “port-access “mitral valve repair and was the beginning of the endoscopic cardiac surgery program at Cardiovascular Institute “DEDINJE” in Belgrade. After a four years break, the program resumed in 2016, and more than 150 port-access heart surgeries were perfumed ever since.
Prof dr Alain Carpentier
Mitral valvuloplasty was implemented and widely accepted during the 1970s, thanks to Dr. Alain Carpentier. Mitral valve repair demonstrated overall superiority comparing to the valve replacement and become the golden standard in mitral surgery. Prof Carpentier, our teacher, and friend, visited Cardiovascular Institute “DEDINJE” in Belgrade, Serbia, several times.
Annuloplasty ring
Annuloplasty ring is a kidney shape device used in mitral valve repair surgery to reduce and reshape the mitral valve orifice. That is the only foreign material implanted and gets covered by heart tissue within three months after the surgery.
Atrial fibrillation
Long-lasting mitral valve disease results in left atrium enlargement and eventually in atrial fibrillation. The atrium is fibrillating rather than contracting, making the blood flow to slow down and clothing within the atrium. Such a thrombus could detach out of the atrium and embolize the peripheral arteries. Therefore, patients in atrial fibrillation must have lifetime anticoagulation therapy. That is why we indicate reconstructive surgery in the early stages of mitral valve prolapse. Otherwise, even in the case of successful mitral reconstruction, patients have to take lifetime anticoagulation drugs due to atrial fibrillation. Atrial fibrillation could be radio ablated during the mitral surgery.
RADIOFREQUENT ABLATION
RF or radio-frequent ablation is a procedure in which the high-frequency waves are used to treat heart arrhythmias. Radiofrequency waves are applied to the heart by a specially designed catheter generating the heat and, therefore, cutting the arrhythmia pathways. That is generally interventional or Cath lab procedure, but could be done as open one during the heart surgery.
Therefore, RF ablation is mainly performed along with the mitral repair surgery due to the high incidence of atrial fibrillation in those patients. If left untreated, the patient has to take anticoagulation drugs even in case of successful mitral repair, which significantly affects the quality of life after the surgery.